
The quest for youth and beauty dates back to centuries ago when Cleopatra allegedly bathed in donkey milk (contains high amount of lactic acid which is an alpha hydroxy acid -AHA) to maintain a youthful clear skin. Cleopatra was not alone in this, the Greeks and French were also using sour milk (lactic acid) and fermented grapes (tartaric acid) for their skin.

These ladies were not wrong in doing so! These centuries old beauty regimes have paved the way for modern anti ageing, and anti pigmentation beauty treatments.
So what does the 21st century beauty treatment look like?
The same concept of using sour milk etc to chemically exfoliate the upper dead layers of your skin is now being performed by dermatologists all over the world as an office based treatment called “chemical peel”.
There are various beauty treatment options available now, from creams, to LASER’s, to botox, fillers and chemical peels being one of them.
What is chemical peel?
Chemical peels are well controlled cosmetic procedures where a chemical with keratolytic property (able to exfoliate the skin cells -keratinocytes) is applied to the face with the aim of accelerating the natural exfoliation process wherein the superficial dead damaged skin is removed thereby improving the texture of skin, the appearance of fine wrinkles and decreases pigmentation.
In layman terms, chemical peels are cosmetic procedures that uses chemicals to peel off the dead layer of the skin.
The depth of such an effect will depend on the type of chemical used and the concentration of the substance ( eg. Glycolic acid- GA 10-30% is a very superficial peel i.e works in the upper epidermis while GA > 30-70% is a superficial peel effecting the lower epidermis and >70% is a medium peel reaching the dermis).
How does chemical peel work?
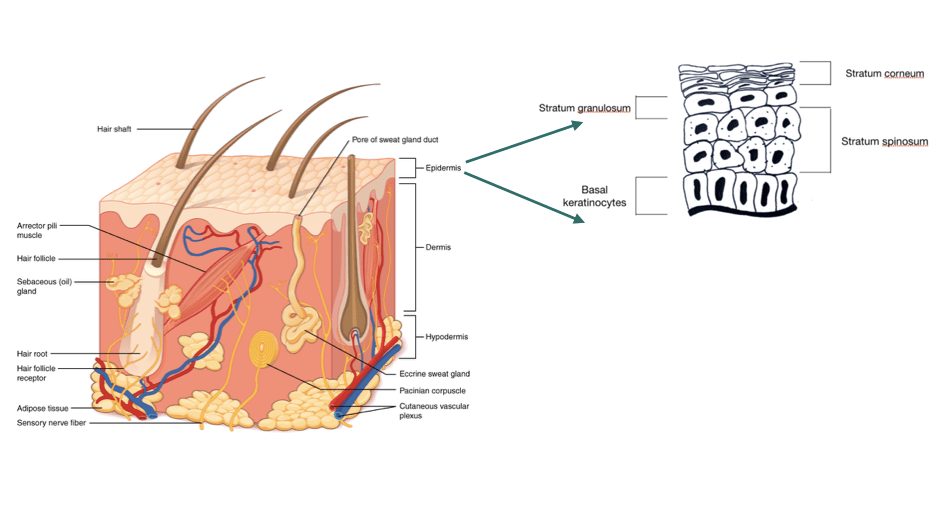
The cells in our skin undergoes a process of multiplication and differentiation (change in shape, structure and biochemical composition) in which cells in the lowermost epidermis change their shape and composition as they move up to the uppermost layer and are eventually shed off.
This is called “skin cell turnover” which normally takes 28-40 days. This turnover is faster in babies and children and slows down with age.
As the cell turnover slows down, the dead skin cells in the uppermost layer of the skin do not get renewed but accumulates and gives the skin a dull, dry and aged appearance.
Ingredients such as alpha hydroxy acids (glycolic acid, lactic acid, mandelic acid etc) disrupts enzymes in the skin that hold the cells together. They can therefore cause the superficial layer of the skin to exfoliate and induce new cell replacement.
At higher concentration, these acids can penetrate deeper into the dermis and stimulate the fibroblast (cells that make collagen) to produce more collagen, elastin and substance that add structure to the skin (GAG’s) thus improves skin thickness and hydration.
Tricholoroacetic acid (TCA) works by causing destruction of the cells by protein denaturation. This then stimulates new wound healing.
Overall benefits that can be achieved with chemical peels
- Improves skin texture
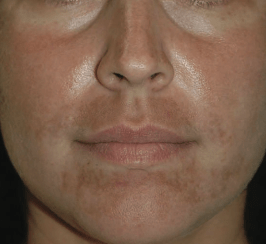
- Can even out skin tone
- Spot peels can be used to treated selected hyper-pigmented areas
- Salicyclic peels are used as an adjunctive treatment for acne
- Improves the appearance of aged skin.




Procedure of a chemical peel
Chemical peels are not meant to work just on their own. One has to be motivated to follow a strict skin care plan for the maximum benefits from such a procedure.
A dermatologist will take a detailed history and clinical examination to assess if a patient is a good candidate for chemical peels.
A patient will be counselled on the skin care measures that needs to followed prior and after the procedure as well as about the expectations from this cosmetic procedure.
A process called “priming” which is done to thin out the epidermis so as the acids used in the chemical peel can penetrate the layers of the skin evenly. This step involves daily application of creams containing either retinoids/ azaelic acid/ kojic acid etc for at least 2-4 weeks prior the chemical peel procedure.
Sunscreens is an absolute must before and after the procedure.
A dermatologist may do a test peel behind the ear or other areas just to check if a patient is allergic to any of the ingredient or to assess for potential side effects.
Chemical peels are done in an office based setting once in a 3-4 weeks for 6-7 sessions depending on a patient’s response. The chosen acid is applied to the entire face or target area using a brush after degreasing the face. The peels are left for a certain contact time which is increased every session ( for eg, for the first session the contact time maybe 2 min which is then increased by a minute or two every successive session).
Post peel care
This step is just as important as the actual peel procedure.
Cold compression using ice packs if there is any redness after the prcedure.
Strict sun protection using broad spectrum sunscreens.
Use mild cleansers or soap free cleansers for washing the face.
Use a moisturiser at least twice daily to help reduce the peeling of the skin.
Avoid facial waxing, threading, facials and skin bleaching procedures for at least 1 week after the procedure.
Avoid scratching, picking or peeling of the skin.
Complications
Chemical peels are not free form side effects, that’s why pre procedure counselling and right patient selection is very important.
The possible side effects are :
- Persistent redness of skin
- Post inflammatory hyper or hypo-pigmentation (i.e dark or light spots)
- Scarring
- Excessive peeling of skin
- Scabbing
- Allergic reactions.
- Scabbing.

Chemical peels are add on cosmetic procedures that can be used for various indications. The effects can be impressive when done by an experienced dermatologist and when a patient is compliant with the pre and post peel skin care.
Never try to attempt a self chemical peel at home with products that can be bought online because the side effects could be permanent if sub optimal products are used and with inexperienced hands.




































{kind=link}
{kind=link}