One common concern individuals with darker skin face is tanning with exposure to UV radiation from the sun. While this is much sought after by people with fair skin, it is not well perceived by brown skin individuals who often desire a tan-free complexion.
why does tanning occur?
Tanning can be of various types and while the exact mechanisms of how tanning occurs still remains elusive, the various types of pigmentary response to UVR exposure seems to have a different underlying reason as to how it happens.
Immediate Pigment Darkening:
This happens within minutes of sun exposure. UVA radiation from the sun causes a chemical reaction ( photo-oxidation) of the pre-melanin pigment present in the melanocytes (pigment producing cells) in our skin.
Persistent Pigment Darkening
This occurs with UVB exposure and is thought to be due to increase activity in the melanocytes which then produces more melanin. The dendrites (finger-like projections of the cells) of the melanocytes extend and branch out more into the surrounding skin-cells (keratinocytes) to transfer their melanosomes (organelles where the melanin pigment is formed and stored) into these cells thus causing the increase visible pigmentation on the skin.

what about a tan that last for months?
For most individuals, once exposure to UVR is discontinued, a skin tan will fade in a few weeks. However, for some a skin tan can last for months even with cessation of sun exposure. This have been recently described in the litterature as “Long-lasting pigmentation”.
Such long-lasting pigmentation could be explain by the following reasons:
How to fade a skin tan?
As discussed earlier, most often a skin tan fades spontaneously after a few weeks. For persistent skin tan addressing the possible reasons for the increase pigmentation could help speed up the fading process.
- Strict sun protection: Skin tanning will continue to occur if there is continued sun exposure. Hence, it is important to follow sun protection measures in the form of either sun protective clothing or regularly using a broad spectrum sunscreen. For sunscreen recommendations, check out my amazon storefront (for Indian options) and my Shop my shelf (for International options).
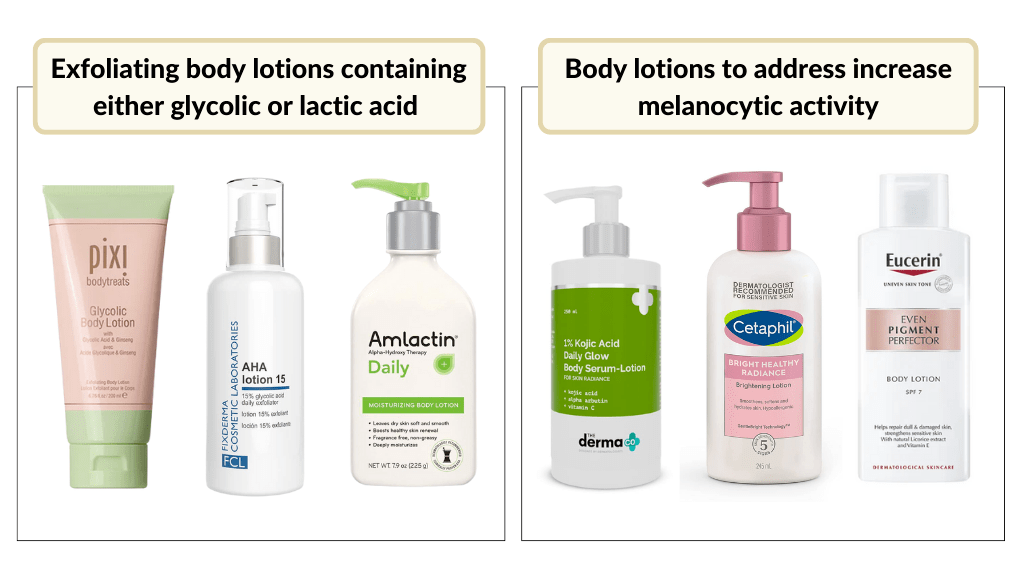
- Exfoliating agents: Products formulated with exfoliating acids such as glycolic acid, lactic acid etc can aid in the shedding of the upper layer of the skin. For body tan, opt for lotion formulation. I advised against using products with high concentrations of such acids that are often formulated for use over smaller areas such as the face for the entire body. For a more detailed post on “exfoliating agents“, head to my earlier blog post on “Acids in Skincare”
- Addressing increase melanocytic activity: Products that help to target pigmentation by by inhibiting the enzyme “tyrosinase” can also help fade a tan faster. Again, if the goal is to fade a tan on larger areas such as legs or arms, lotion formulations are the best.