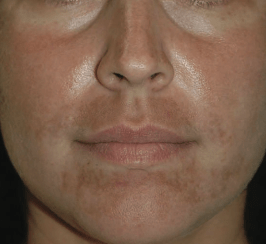
Sunscreens are the number one skin care product every dermatologist swears by. In the Western countries, where the incidence of sunburns and skin cancers are high among Caucasians, sunscreen is life saving. In a country like India, where the individual’s skin type (FST IV and V) predisposes them to pigmentation disorders (melasma, post inflammatory hyperpigmentation -PIH), sunscreens are the first armour to fight against pigmentation.
Lets recap a little on solar radiation, so as to understand what exactly a sunscreen does.
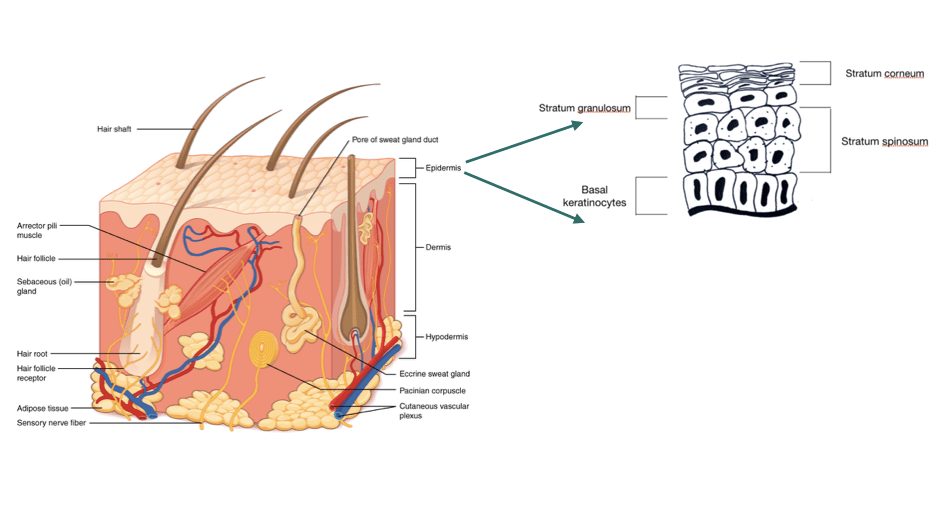
UVA– 98-99% of the solar radiation reaching the earth’s surface. UVA is the spectrum of UV radiation that can penetrate the dermis and is responsible for immediate tanning, photoaging, pigmentary disorders, photodermatoses such as polymorphous light eruption etc
UVB– 1-2% of UVR reaching the earth’s surface. UVB is highly energetic but does not penetrate beyond the epidermis (superficial layer of skin) and is responsible for sunburns, skin cancers and delayed tanning. UVB is also required for Vitamin D synthesis in our body.
UVC– filtered out by the ozone layer and does not reach the earth’s surface.
How sunscreens work?
There are two types of sunscreen :
Physical or inorganic sunscreens
They contain titanium dioxide, zinc oxide, iron oxide, or calamine, and functions by forming a coat on the skin that reflects, scatter or absorb the UVR. Physical sunscreens are ideal for patients with sensitive skin as the ingredients do not interact with the proteins and lipids in the skin, and they can protect against both UVA and UVB radiation but they bear the disadvantage of leaving a white cast on the skin. The newer physical sunscreens are relatively more expensive as well.
Micronised & ultrafine particles of zinc or titanuim oxide are generally considered more acceptable cosmetically. Multiple positive reviews on elta MD and LRP physical sunscreen, consumers remarked that these sunscreens do not leave white cast and blends easily.
Neutrogena and kiehl’s have mixed reviews. They seems to be well suited for fair skin individuals and not very aesthetically pleasing to individuals with darker skin tone.
Chemical or organic sunscreen
Most sunscreens available in the market are chemical sunscreens. They contain ingredients that can absorb UVR and converts it to heat energy which then dissipates into the environment. They do not leave a white cast on the skin and hence considered more cosmetically acceptable.
Chemical sunscreens are most commonly found in the market. Bioderma photoderm max has a combination of both physical and chemical sunscreen and no white cast on application.
Active ingredients in chemical sunscreens
It is not uncommon to find a mixture of both physical and chemical sunscreen as well. The disadvantage of a chemical sunscreen is that the active ingredients can react with components in the skin such as proteins and lipids which then may result in wanted production of reactive oxygen species causing irritation to the skin. Susceptible individuals may be sensitized to these components in the sunscreen which will manifest as contact allergic dermatitis (red, itchy skin). For this reason physical sunscreens are preferred for patients with sensitive skin.
What does SPF and PA factor mean?
SPF stands for sunburn protection factor which is a measure of protection against UVB induced sunburn. Sunscreen which only mentions SPF means they only provide protection against UVB and not UVA ( the spectrum which is responsible for pigmentation, photoaging). The grading of SPF is as follows:
- Low: SPF 2 – 15
- Medium: SPF 15 – 30
- High: SPF 30 – 50
- Highest: SPF >50
An SPF of 15 blocks 93% and an SPF of 30 blocks 95% of the UVB radiation. Note that double the SPF does not mean double the protection. Sunscreens with higher SPF contains more active ingredients which may make the product less pleasing to use to some individuals.
PA factor measures the protection against UVA. It measures the Persistent pigment darkening (PPD) or tanning after UVA exposure.
- PA + : some protection from UVA
- PA ++: moderate protection
- PA +++: best protection
- PA ++++: highest protection : rare to find this in products
How to use a sunscreen?
A given sunburn protection factor in a sunscreen can be obtained only when the right amount of sunscreen is used. Studies use 2mg/cm2 when testing for SPF in a sunscreen, however in reality we tend to use a lesser amount which will then result in a lower SPF than what is labelled in the sunscreen. Therefore dermatologist recommend a higher SPF (SPF>30) to help compensate for the inadequate application.
Dermatologist use the “teaspoon rule” to determine the correct amount of sunscreen needed.
- 3 mL (slightly more than half a teaspoon)- 3 mL for each arm and 3 mL for the face and neck
- 6 mL (slightly more than a teaspoon)- 6 mL for each leg, 6 mL of the chest and 6 mL for the back
Apply a sunscreen at least 20 mins prior to outdoor exposure so as the ingredients can form a uniform layer on the skin. It is also ideal to wait 20 mins before putting on clothes otherwise a significant amount of sunscreen will be wiped away during the contact with clothing. The best way to do this is to apply a sunscreen right after a shower or washing your face in the morning and not wait until its time you get dressed for work.
When to re-apply a sunscreen?
We are all familiar with the golden rule of “re-application of sunscreens” which states that a sunscreen must be re-applied every 2 hours as physical activities like touching your face, sweating, friction from contact with sand at the beach can remove some amount of sunscreen from your skin. Reapplication is also recommended after activities in water.
So does this rule apply to modern water-resistant sunscreens which can bind effectively to the skin and retains its said SPF even after 40-80 mins immersion in water?? Recent studies have shown that reapplication helps compensate for the under application of sunscreens. Reapplication after 20 mins also provides better protection against sunburn than delayed reapplication i.e after 2 hours. Therefore early reapplication of a sunscreen is preferred, ideally within the first hour of the first application.
Gentle application is better for sunscreens with gel, or creams consistency. Rubbing it immediately on the skin is recommended for spray sunscreens.
Always search for a broad spectrum sunscreen (UVA & UVB protection) and a water resistant sunscreen.
White cast of physical sunscreens.
The white cast blends with the skin in 30-40 secs of gentle rubbing.
Aesthetics of chemical sunscreens
No white cast, no excuse. Wear sunscreen.
Scientific evidence of the effectiveness of sunscreens for melasma in Indian patients.
A recently published study in the Indian journal of dermatology which studied the efficacy of two different sunscreens on skin pigmentation. A total of 230 patients were recruited in the study. One group was given a sunscreen with an SPF of 50 with PA +++ and the other group a sunscreen of SPF 19 and PA +++. At the end of 12 weeks of twice daily usage, a significant improvement in the form of decrease density of pigmentation and better radiance was noted in both groups. The conclusion is that:
Regular use of a sunscreen with high UVA protection (PA+++) highly effective in improving the skin radiance and in decreasing the skin pigmentation.
So my advised is always look for a sunscreen with PA+++ if you have pigmentation issues, and if you are also prone to sunburns, then get one with an SPF of at least 30.
Hope this was helpful. And stay tune to my next posts on “Controversies regarding sunscreens”.


















































{kind=link}
{kind=link}