I’ve written post on this a while ago, and not much data was available then regarding truncal acne.
So here’s an update on another common issue : Truncal acne.
Truncal acne refers to the acne involving the back and or chest. Around 50% of patients with facial acne also suffer from truncal acne while ~ 3% suffer from just truncal acne without any acne on their face.
How is it different from facial acne?
Truncal acne has been neglected in comparison to facial acne. Not much studies are available on this entity and treatment options are limited as well. Creams or gel that are available for face may not be enough or prove to be too costly for application over large surface areas such as the back or the chest.
Triggers for truncal acne
Triggers are external factors that could cause development of acne in genetically predisposed individuals.
Whey protein supplements have been reported to cause acne eruption in body builders
How is body acne treated?
In general, treatment of truncal acne follows the same principles as for facial acne.
The only difference is that one needs to be mindful for the choice of products for truncal acne. A small 15g cream or gel may prove to be too costly as it may not be enough to treat large surface areas such as the back and chest.
Lotion or foam formulation may be a better and more convenient choice for the back/chest.
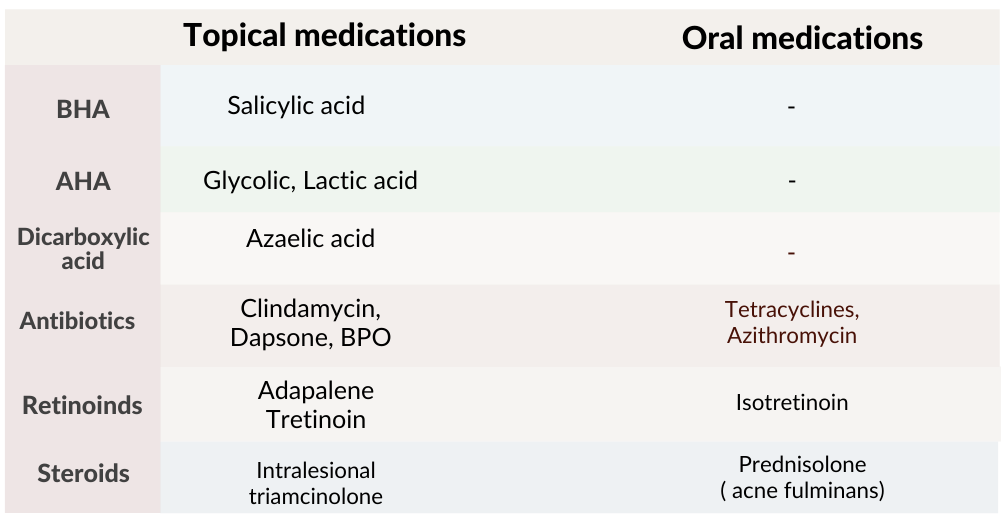
Few are available as over the counter (OTC), while medications such as antibiotics, retinoids or steroids require prescription and supervision by a dermatologist
When in doubt of the diagnosis and how to use these products
If you have a personal history of developing hypertrophic or keloidal scars (thick, large scars), early treatment will help prevent such scar formation
Severe extensive involvement may require a course on antibiotics or isotretinoin
Managing post truncal acne scars either atrophic, hypertrophic or pigmented scars may require in office procedures such as chemical peels or LASERS, etc
Post acne erythema are also called post acne erythema or macular erythema.
They are persistent pink to red marks that occurs in acne patients during the course of acne treatment and persists for sometime even after the acne subsides.
They are more commonly seen in patients with lighter skin (FST I-III), but PIE can also be seen in Indian skin type FST III & IV as well.
PIE is a relatively new term, which is different from post inflammatory hyperpigmentation (PIH) i.e the brownish black scars that follows an acne eruption.
Difference between PIH and PIE
How and why does PIE occurs?
Still not clearly understood. Potential explanation is that during the process of inflammation, some pro-inflammatory cytokines that are released causes dilatation of the small blood vessels present in the superficial most part of the dermis.
The epidermis while still being in the process of maturation, is thinner, more transparent and can thus more incident light is reflected from the underlying vasculature
So far, there is not much options for treating PIE.
The best approach is to minimise the risk of developing PIE in the first place.
As blood vessels will dilate during the process of healing, so some amount of erythema (redness) is expected. However as persistent inflammation is the driving force for long lasting erythema seen as PIE, addressing the factors that causes the inflammation will help minimise the chances of developing persisting PIE.
You do not need to buy products with these individual ingredients separately. Just look for products formulated with these ingredients together either in your moisturiser or sunscreen
Treatment that have been tried for PIE
For most individuals with acne, PIE subsides spontaneously after a few weeks to months just with gentle, supportive care in the form of sunscreens, moisturisers +/- ingredient to help with the inflammation.
However for some, PIE can be persistent even with the above measures. Medical management that have been tried include topical creams and different types of LASERS.
There is still no standard treatment for PIE and large scale studies are still lacking
So far, LASER treatment is still the best option for persistent PIE
Do you often get your breakouts just before one event? Have you ever used Pimple patches? What is these patches made of? Do they even work? Can they work for all types of pimples?
What are pimple patches?
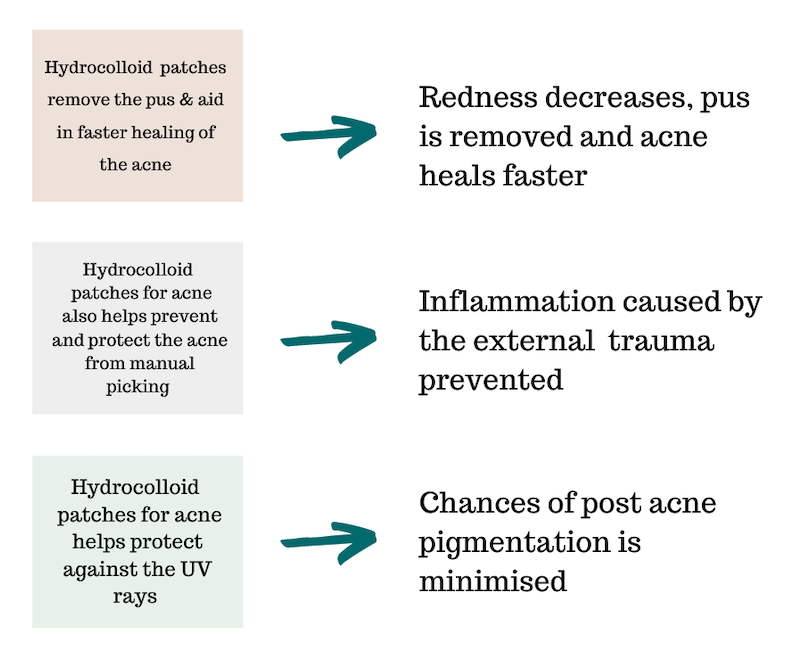
These patches are hydrocolloid dressings which were traditionally used for treating acute or chronic wounds. They’ve also been used for the management of post surgical wounds.
Hydrocolloid are hydrophilic (water loving) substance composed of gelatin, pectin, carboxy-methylcellulose. As these substances are attracted to water, they are they can absorb water, and pus from the wounds and then forms a gel which provides a moist environment for the wound.
How do hydrocolloid help in wound healing?
How do hydrocolloid dressings work for acne?
Which type of acne are they best used for?
Single or limited acne
Perfect as an SOS solution for those pimple that always pop up before an event.
Acne which is inflamed (red, painful, with or without pus)
Pimple patches are not ideal for severe, cystic acne.
How to use pimple patches?
Wash face clean before application
Apply the patches over the acne on dry, clean skin
The patches can be left overnight or longer (12-48hrs)
Dispose used patches. Do not reuse them
Skip using face serums, moisturisers oven the active acne before applying the patches
The patches are transparent so they be used during the day.
These patches do not replace the regular acne medications such as benzoyl peroxide, adapalene etc. They serve as rescue treatment for those once in a while acne breakouts.
Are there any concerns regarding these patches?
Well as great as they seem in theory as the emergency acne rescue option, there have not been much research done for their use in acne. I would love to see more studies comparing these to spot application with benzoyl peroxide or salicylic acid.
Some individuals may even be allergic to either the adhesives used in these patches or other ingredients.
So in conclusion:
If spot application of benzoyl peroxide works for you, continue it. There is no need to buy spend extra money on these patches. But if your skin gets too irritated or dry with actives such as benzoyl peroxide or salicylic acid, or you’re the type that just can’t control picking on your acne, then these patches could be a great option for you.
Pimple patches available in the Indian market
Pimple patches are available as either pre cut patches or as single sheets for a customisable size. One can make heat shapes or star shapes or whichever fun shapes out of these sheets.
Some pimple patches also contains active anti acne ingredients such as salicylic acid, tea tree or cantella asiatica which helps in calming and soothing the skin.
These are available at either amazon or on flipkart
Acne is such a common condition that to an untrained eye, all red bumps (papules/pustules) must be acne.
There are other dermatological disorders that present like acne but are not acne.
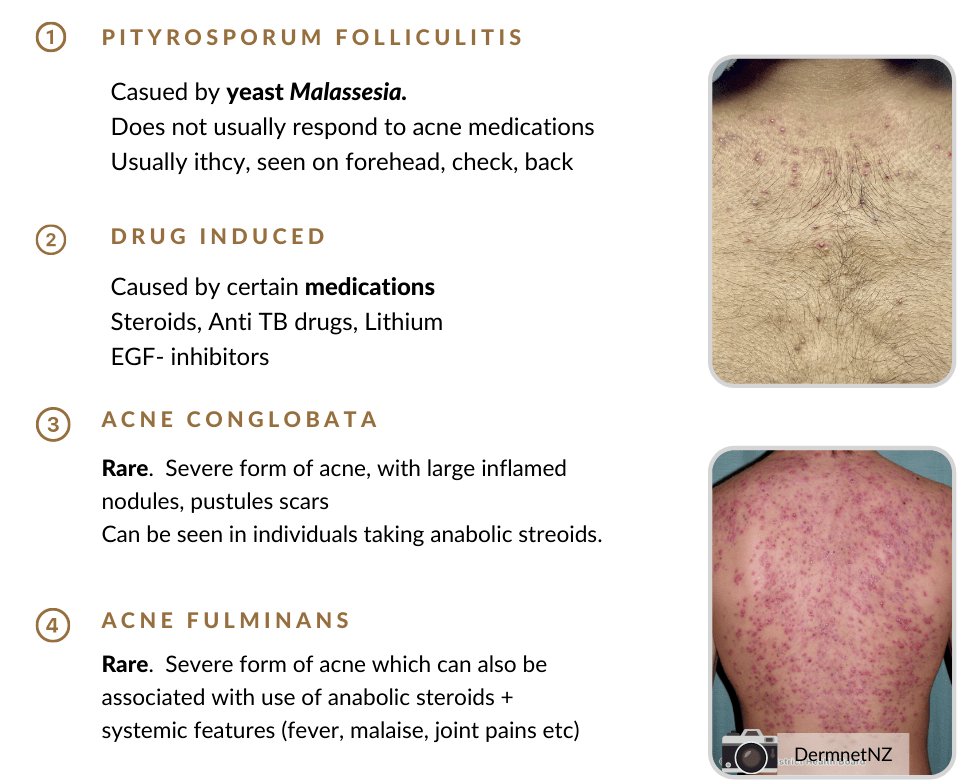
Pityrosporum folliculitis or Malassezia folliculitis (Fungal acne in layman terms, but fungal acne is not a medical diagnosis since it’s not acne or form of acne) is one of the most common skin condition mistaken for acne. It is caused by increase colonisation (multiplication) of a yeast called Malassezia species which is normally present as part of the normal flora in our skin. (yes! our skin has a world of micro organisms living in it 😉 )
It is the inflammation caused by such an increase colonisation that causes the symptoms.
So what causes this increase colonisation by this yeast?
Malassezia thrives in the oily environment produced by the sebaceous glands. Adolescents (10-19 years) have an increase sebaceous glands activity due to the hormonal fluctuations. Therefore this condition is commonly seen in adolescents.
Excessive sweating is also a risk factor, and people living in hot humid areas are more predisposed.
Individuals on topical or oral antibiotic, as this can suppress the growth of the normal bacteria in the skin giving way for this yeast to multiply unchecked.
Use of steroids or other immunosuppressant agents.
Diabetic patients may also experience such eruptions.
Genetic predisposition also plays a role. As mentioned earlier everyone has this yeast in their skin, but only some people are able to mount an inflammatory response to it causing the symptoms while others do not.
How can you differentiate it from acne ?
Firstly by the looks of the lesion, fungal acne presents with monomorphic (uniform looking) papules (red raised bumps) or pustules (pus filled bumps). There will not be any comedones (such as white heads or black heads) unless a patient also has concurrent acne.
Secondly by examining the site of involvement, face (forhead), back, upper arms, chest and back are involved in fungal acne. One wouldn’t normally see acne vulgaris involving the upper arms, neck.
Thirdly, fungal acne tends to be itchy while acne is not. Do you ever remember your pimple itching unless you’ve picked on it and a scab has formed?
Fourthly, history of acne not responding to anti acne treatment despite strict compliance or acne which had responded to treatment and suddenly flares up even while on the same treatment.
Fifthy, individuals with fungal acne may also have dandruff or tinea versicolor.
Do you need to see a dermatologist for such a condition?
Its always better to get an expert opinion before you self treat any skin condition.
Though the above points can help distinguish between acne and fungal acne, it may not be as clear cut in most cases, especially when one also has co existing acne. A variant of acne called truncal acne vulgaris can also present with similar eruptions on the back and chest.
Another dermatological condition called acneiform eruption which presents as eruption of skin lesions similar to acne caused by certain medications, mechanical friction, certain compounds used in textile dyes, insecticides, pesticides, detergents or soaps (halogenated aromatic hydrocarbon) presents similar to acne, and is sometimes difficult to differentiate it from fungal acne.
This is where a dermatologist’s opinion is important, so that certain questions can be asked, and if necessary certain tests performed (such as Wood lamp examination or KOH mount which can help in the diagnosis of fungal acne) for the correct diagnosis and management of the condition.
How to treat it?
As it is seen that the organism causing fungal acne (i.e Malassezia sp) can multiply more in hot and humid areas and summers are the season for most flare ups due to the increase ambient temperature and sweating, measures to reduce these factors can help reduce the symptoms
Have frequent cold showers in the summers
Change clothing such as gym wear, uniforms as soon as possible
Opt for loose fitting clothing
Avoid tight fitting attire
Seek the comfort of an air conditioned room
Products to use :
Use an anti-fungal shampoo (such as 2% ketoconazole or selenium sulfide or zinc pyrithione), look out for these ingredients in your anti dandruff shampoos. (List of few of such shampoos on previous post)
2% Ketoconazole + zinc pyrithione
Zinc pyrithione
Zinc pyrithione
Massage the shampoos to the affected areas and leave it for 5-10 mins and wash off. This can be done twice weekly for at least 2-4 weeks depending on your response.
If the above fails, your dermatologists may add topical anti-fungal creams which are to be applied once-twice daily over the lesions.
Topical creams that helps to unclog the blocked sebaceous glands such as salicycic acid is another adjunctive treatment option in addition to the above.
Systemic anti-fungals (oral tablets/capsules) may be required in some cases.
Remember that the condition may recur, especially in summers.
Applying the anti-fungal shampoos during the summer months once weekly even if you don’t have the flares may help reduce chances of recurrence