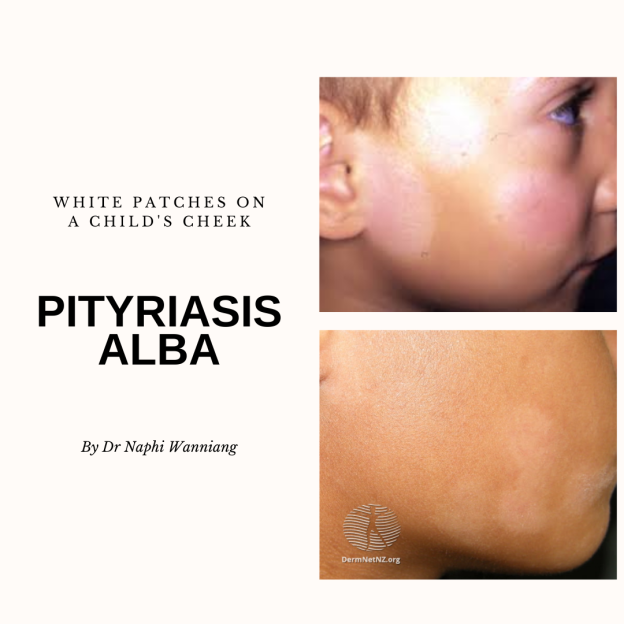
First stage : Starts as areas of mildly erythematous (red) patches on the cheeks or chin, or arms. It may be itchy at this stage. This stage is commonly more noticeable in fair skin individuals and often missed in darker skin individuals.
Second stage : The erythematous patches subsides leaving behind pale hypo-pigmented patches with the fine scaling on the surface. This is more prominent in darker skin tones and it is usually at this stage that parents seeks medical attention for the patches.
Third stage: The pale patches spontaneously subsides in a few months to years leaving no scars
Variants of P.alba
Should I be worried that my child has P.alba?
No, P.alba is a benign self resolving condition. The patches subside spontaneously within a few months or years for some without any sequelae.
It is important to remember that it may take years to complete resolution of the patches of P.alba in few patients.
Why do you need to see a dermatologist?
P. alba can mimic many other skin conditions, therefore getting an expert to examine the skin lesions for a proper diagnosis is of utmost imporatance.
You dermatologist can help conduct certain bedside test on the skin to help rule out the above mentioned conditions.
Once the diagnosis of P. alba is ascertain, the dermatologist will advised on your skin care and treatment accordingly depending on the stage of the condition.
What one can do to help improve the appearance of the skin lesions:
Avoid excessive bathing and excessive washing and scrubbing of face
Use moisturisers, it helps improve the appearance of the dry scaly patches
Always use a broad spectrum sunscreen which will help prevent further tanning and darkening of the surrounding skin, thus minimising the contrast between the pale patches and the neighbouring tanned skin.
What your dermatologist may prescibe?
A Short course of mild topical steroids especially during the first stage of the disease when the rash erythematous and itchy.
Topical calineurin inhibitors such as tacrolimus or pimecrolimus during the second stage.
I recently visited my hometown, Shillong in the north eastern part on India during the last few days of November and it was already cold especially at night. The water was freezing cold as well.
The first thing I noticed was my skin felt extra dry, with visible patches of dry spots. My lips were constantly chapped and I could literally write on the skin on my legs. These skin changes were happening with everyone. My family members and I had patients from back home that all complaint that their skin felt tight.
So why does this happen in winter?
To understand this, we will have to do a deep dive into how our skin functions in an optimal environment.
As you can see the protein filaggrin plays an important role in hydrating the skin, protection against UV rays and maintaining a healthy skin barrier. Individuals with mutation in the gene encoding filaggrin protein are more predisposed to developed eczemas and other allergic conditions such as asthma. Studies have found that low humidity and low temperature causes a decrease in the amount of natural moisturising factor (NMF) in the stratum corneum and this causes decrease in skin hydration. This results in the subjective feeling of dry flaky skin during winters.
Animal studies also show that when the skin is exposed to low humidity, a reactive pathway favouring pro inflammation is activated within 24 hours. What this means clinically is that, the skin maybe more sensitive to ingredients present in skin care products during winters.
Certain skin conditions can worsen during winters. Individuals suffering from eczema, psoriasis, rosacea, cold urticaria should be careful not to be exposed to cold weather, water and to aggressively take care of the skin by moisturising and being gentle with their skincare.
Skin changes associated with using radiation heaters during winters
Homes in Shillong do not have central heating and rely on the use of radiation heaters or coal stoves to keep them warm. There are certain skin changes that can be associated from exposure to such infrared radiation.
Erythema ab igne/ Toasted skin syndrome/Fire stains
Reticulate (lacy pattern) erythema (redness) and pigmentation on the skin caused by chronic and repeated exposure to infrared radiation from heaters, wood or coal stoves. This has recently been described to be seen on the thighs of people with prolonged contact with laptops.
Though the condition is benign and resolves when the heat source is removed, the pigmentation can be permanent for some and in rare instances skin cancers such as squamous cell carcinoma or merkel cell carcinoma can develop.
Avoid sitting too close to the heat source (heater or stove)
Wear protective clothing to prevent direct exposure of the skin to the heat radiation
Remove the most heat source the moment redness develops on the skin
Seek a dermatological examination if a non-healing ulcers or wound develops over the skin where the pre-existing erythema or pigmentation was.
Worsening of Melasma
A multi centric cross-sectional study from India found a significant and positive association with the duration of heat exposure and the severity of melasma
If you suffer from melasma, avoid sitting too close to the heat source and always remember to wear a broad-spectrum sunscreen even when indoors.
Parabens have been been used since the 1920s safely as preservatives in skin care products, cosmetics and various other toiletries items used in our every day life. Parabens are also present in certain food such as blueberries, strawberries, grapes, barley etc though in small quantities. Parabens are also used in pharmaceutical companies in various medications. Even though they’ve been around for 70 years, parabens still remains a controversial ingredients in the skin care industry. They were first victimised as sensitisers that are able to cause contact allergic dermatitis. In the recent years, parabens are again under scrutiny as potential endocrine disruptors acting as the hormone estrogen. They have also been falsely linked to breast cancer and infertility.
Now let’s see if all these claims are true! Before we dive into the research available on parabens, let’s understand a little background on these molecules and how the processed inside our body.
Background on paraben
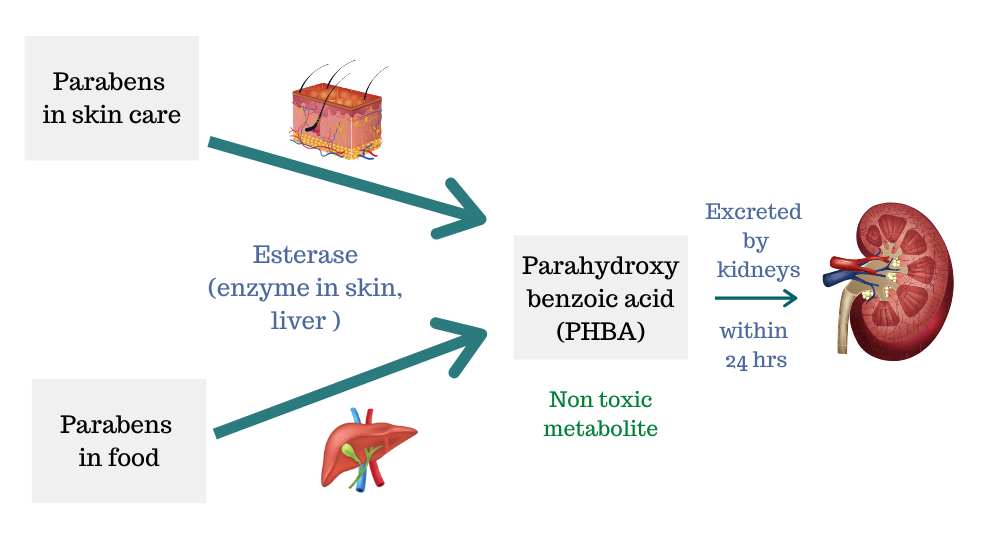
Parabens are esters of parahydroxybenzoic acid (PHBA). There are different classes of parabens: methyl, ethyl, butyl, and propyl – paraben are the four most commonly used ones with a good track record.
Metabolism of parabens
Why are parabens present in skin care products and cosmetics?
Effective antimicrobials at even low concentrations hence acts as preservatives.
Minimal toxicity
Chemically inert
Odourless
Low cost
pH neutral
They have been used safely since the 1920s as have been extensively studied for the safety profile in humans
With such advantages properties, a number of skin care products, cosmetics contain paraben as the choice of preservative.
Parabens as sensitisers
Parabens were labelled as contact sensitiser i.e Able to cause contact allergic dermatitis when applied to the skin. However, cases of paraben allergies have been consistently low with parabens being the culprit in only ~0.6 to 1% of the individuals with contact allergic dermatitis.
Most of these paraben allergies occurs in individuals with compromised skin barrier such as when products containing parabens were applied on eczematous or wounded skin.
An interesting observation called “PARABEN PARADOX” in which the same above individuals who reacted to paraben when applied to compromise skin, didn’t have any problems with the same paraben containing cream was applied to normal skin.
Parabens were even named the contact non-allergen of the year in 2019 by the American contact dermatitis society. Parabens are also the least allergenic preservative present in the market
Parabens as endocrine disruptors
It has been shown in vitro studies (lab studies) that parabens are able to bind to estrogen receptors. Amongst the various parabens, butyl paraben has the highest oestrogenic activity but overall has a weak oestrogenic potential and is 10,000 times less potent than the naturally present hormone estradiol. When lab animals was subcutaneously injected with high dose of paraben it was shown to cause increase in the size of the uterus. Though these findings may seem alarming, they do not represent the effects of parabens in humans.
Though parabens may act as endocrine destructors in vitro, there is no evidence that they are endocrine disruptors in humans.
Paraben linked to breast cancer
As paraben and can mimic estrogen and bind to estrogen receptors, there is a theoretical risk that they could increase the risk of breast cancer. However as stated earlier, parabens have only a weak oestrogenic activity. Even if they can bind to these estrogen receptors, there is no evidence that it can produce any effects in humans. Another reason why parabens are linked to breast cancer is because some studies were able to isolate parabens from cancerous breast tissues. But most of the studies came that came to this conclusion did not assess the presence of parabens in normal breast tissue.
One study found that parabens were present in the adjacent normal breast tissue as well.
One epidemiological study reported no increased risk of breast cancer incidence in patients using antiperspirant or deodorants. However details on the composition of these products were lacking from this study.
So far, there is still no convincing evidence that parabens increases the risk of breast cancer.
Parabens and infertility
Consequences of demonising parabens
With companies being forced to cater to a market that embraces “Paraben free“, alternative preservative with lesser known properties and effects on humans are being used instead.
Avoiding the use of preservatives in cosmetics and skincare products is dangerous as this provides a favourable environment for micro organisms to grow which can result in various skin infections.
Skin care marked as “paraben free” are more expensive due to the use of other more expensive preservatives and because “paraben free” is a great marketing strategy. This would prove to be too expensive for patients who depend on moisturisers or other products to help maintain a healthy skin especially in countries like India.
For these reasons use of parabens have not been banned from cosmetics or skincare products as the benefits of these molecules far out weighs their theoretical in vitro or animal studies risks
I am not saying that parabens are 100% safe, and completely risk free, because nothing on earth is risk free. The best approach in such situation is to try to understand the available data and to weigh the benefits against the risk.
So who should use “paraben free” products?
Individuals with a known allergy to parabens should opt for paraben free products. or if paraben free is your personal choice.
Michelle from Lab Muffin, who talks about the science of beauty, wrote such a great blog posts on this topic as well. Do check that out for an even detailed read.
Do you often get your breakouts just before one event? Have you ever used Pimple patches? What is these patches made of? Do they even work? Can they work for all types of pimples?
What are pimple patches?
These patches are hydrocolloid dressings which were traditionally used for treating acute or chronic wounds. They’ve also been used for the management of post surgical wounds.
Hydrocolloid are hydrophilic (water loving) substance composed of gelatin, pectin, carboxy-methylcellulose. As these substances are attracted to water, they are they can absorb water, and pus from the wounds and then forms a gel which provides a moist environment for the wound.
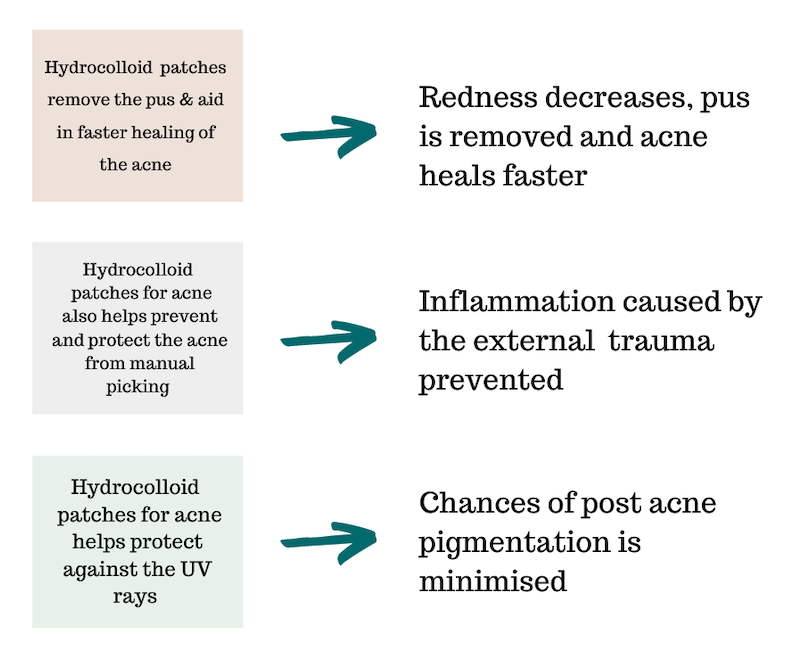
How do hydrocolloid help in wound healing?
How do hydrocolloid dressings work for acne?
Which type of acne are they best used for?
Single or limited acne
Perfect as an SOS solution for those pimple that always pop up before an event.
Acne which is inflamed (red, painful, with or without pus)
Pimple patches are not ideal for severe, cystic acne.
How to use pimple patches?
Wash face clean before application
Apply the patches over the acne on dry, clean skin
The patches can be left overnight or longer (12-48hrs)
Dispose used patches. Do not reuse them
Skip using face serums, moisturisers oven the active acne before applying the patches
The patches are transparent so they be used during the day.
These patches do not replace the regular acne medications such as benzoyl peroxide, adapalene etc. They serve as rescue treatment for those once in a while acne breakouts.
Are there any concerns regarding these patches?
Well as great as they seem in theory as the emergency acne rescue option, there have not been much research done for their use in acne. I would love to see more studies comparing these to spot application with benzoyl peroxide or salicylic acid.
Some individuals may even be allergic to either the adhesives used in these patches or other ingredients.
So in conclusion:
If spot application of benzoyl peroxide works for you, continue it. There is no need to buy spend extra money on these patches. But if your skin gets too irritated or dry with actives such as benzoyl peroxide or salicylic acid, or you’re the type that just can’t control picking on your acne, then these patches could be a great option for you.
Pimple patches available in the Indian market
Pimple patches are available as either pre cut patches or as single sheets for a customisable size. One can make heat shapes or star shapes or whichever fun shapes out of these sheets.
Some pimple patches also contains active anti acne ingredients such as salicylic acid, tea tree or cantella asiatica which helps in calming and soothing the skin.
These are available at either amazon or on flipkart
Aluminium has been shown to possess some undesirable biological effects on human body and exposure to high doses of aluminium has been linked to an increased risk of breast cancer and Alzheimers’s Disease.
Why did the controversy exist between breast cancer and antiperspirant?
As a majority of breast cancer occurs in the upper outer quadrant of the breast it was theorised that regular use of underarm cosmetics such as antiperspirant could potentially contribute to the increasing number of breast cancer detected in this site.
It was also shown in some studies that a concentration of aluminium was found in breast cancer tissues.
In vitro ( laboratory) studies have shown that aluminium can cause DNA instability and can promote cellular proliferation thus could potentially cause cancer.
What do the recent human studies say?
Many studies support the fact that the higher amount of breast tissue present in the upper outer quadrant of the breast is the reason for the increase number of breast cancer detected in this area and not because of it being in close proximity to the axilla (under arm).
Other studies have also shown that aluminium was found to be equally present both in the cancerous tissue as well as normal breast tissue.
The absorption of aluminium present in antiperspirant through the intact skin is very minimal and not significant enough to cause breast cancer.
Systematic analysis of two case-control studies has found no association between the use of antiperspirant and increase risk for breast cancer.
Does aluminium in antiperspirant cause Alzheimer’s disease?
A possible link between aluminium and Alzheimer’s disease was questioned when laboratory studies of high doses of injected aluminium was shown to cause neurofibrillary tangles (characteristic of Alzheimer’s disease)in rabbit brains i.e aluminium is neurotoxic to animal brains. This finding dates back to 1965, and years later it still remains a controversy.
Studying the association between aluminium and Alzheimer’s disease (AD) has been difficult due to the ethical issues in obtaining brain tissue for biopsies. The study so far have been based on autopsied brain specimens from patients with AD. This does not answer whether the increase aluminium concentration found in these specimens were the cause of the disease or a consequence of it.
As Alzheimer’s disease is a chronic disease, prospective studies aiming to determine the association between exposure to aluminium and the disease are met with many hurdles. AD Causes significant memory loss (dementia), studies relying on patients account of their history of exposure to aluminium in the past for example use of aluminium-based antiperspirant are biased, as patients are unable to recall correctly such exposures. Few studies have relied on the accounts given by the patient’s partners who may not have a correct idea of such exposures.
Therefore the association between aluminium exposure be it from our diet or water or underarm cosmetics and Alzheimer’s disease will always be a controversy yet to be proven.
What we know so far?
As stated earlier aluminium present antiperspirant is not significantly absorbed through the skin. The minimal amount that is absorbed is effectively excreted via the kidney before reaching the brain.
Therefore antiperspirant use is not likely to cause Alzheimer’s disease.
Presently there is no strong scientific evidence linking exposure to aluminium (including aluminium in anti-perspirant) as a causative factor To the development of Alzheimer’s disease
The quest for youth and beauty dates back to centuries ago when Cleopatra allegedly bathed in donkey milk (contains high amount of lactic acid which is an alpha hydroxy acid -AHA) to maintain a youthful clear skin. Cleopatra was not alone in this, the Greeks and French were also using sour milk (lactic acid) and fermented grapes (tartaric acid) for their skin.
Elisabeth Taylor as the beautiful Cleopatra
These ladies were not wrong in doing so! These centuries old beauty regimes have paved the way for modern anti ageing, and anti pigmentation beauty treatments.
So what does the 21st century beauty treatment look like?
The same concept of using sour milk etc to chemically exfoliate the upper dead layers of your skin is now being performed by dermatologists all over the world as an office based treatment called “chemical peel”.
There are various beauty treatment options available now, from creams, to LASER’s, to botox, fillers and chemical peels being one of them.
What is chemical peel?
Chemical peels are well controlled cosmetic procedures where a chemical with keratolytic property (able to exfoliate the skin cells -keratinocytes) is applied to the face with the aim of accelerating the natural exfoliation process wherein the superficial dead damaged skin is removed thereby improving the texture of skin, the appearance of fine wrinkles and decreases pigmentation.
In layman terms, chemical peels are cosmetic procedures that uses chemicals to peel off the dead layer of the skin.
The depth of such an effect will depend on the type of chemical used and the concentration of the substance ( eg. Glycolic acid- GA 10-30% is a very superficial peel i.e works in the upper epidermis while GA > 30-70% is a superficial peel effecting the lower epidermis and >70% is a medium peel reaching the dermis).
How does chemical peel work?
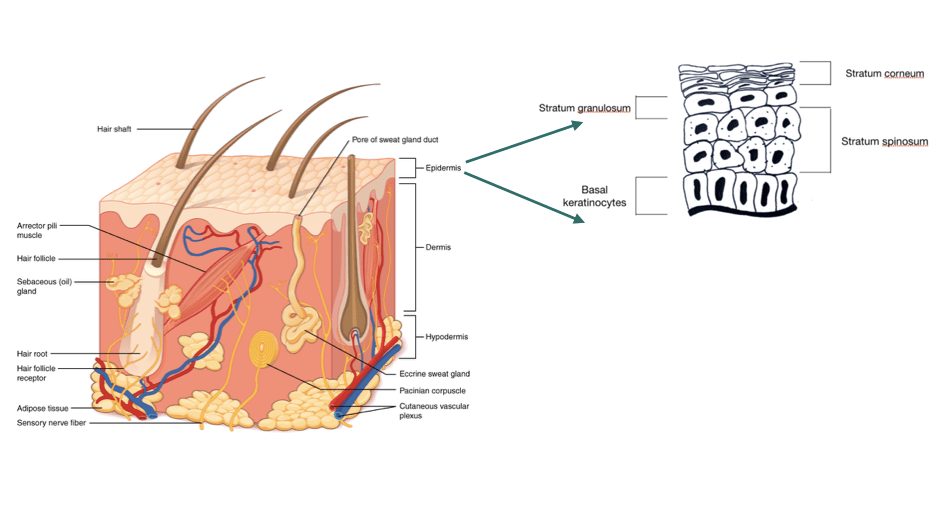
The skin has 3 layers : epidermis (uppermost) , dermis (middle) & sunbcutaneous fat (lowermost). The epidermis itself is divided into 4 layers (basal layer, stratum spinosum, stratum granulosum and the statum corneum.
The cells in our skin undergoes a process of multiplication and differentiation (change in shape, structure and biochemical composition) in which cells in the lowermost epidermis change their shape and composition as they move up to the uppermost layer and are eventually shed off.
This is called “skin cell turnover” which normally takes 28-40 days. This turnover is faster in babies and children and slows down with age.
As the cell turnover slows down, the dead skin cells in the uppermost layer of the skin do not get renewed but accumulates and gives the skin a dull, dry and aged appearance.
Ingredients such as alpha hydroxy acids (glycolic acid, lactic acid, mandelic acid etc) disrupts enzymes in the skin that hold the cells together. They can therefore cause the superficial layer of the skin to exfoliate and induce new cell replacement.
At higher concentration, these acids can penetrate deeper into the dermis and stimulate the fibroblast (cells that make collagen) to produce more collagen, elastin and substance that add structure to the skin (GAG’s) thus improves skin thickness and hydration.
Tricholoroacetic acid (TCA) works by causing destruction of the cells by protein denaturation. This then stimulates new wound healing.
Overall benefits that can be achieved with chemical peels
Improves skin texture
Can even out skin tone
Spot peels can be used to treated selected hyper-pigmented areas
Salicyclic peels are used as an adjunctive treatment for acne
Improves the appearance of aged skin.
Melasma after medium depth peel (Jessner’s solution) Image : Rooks textbook of dermatology
Acne scars after medium depth chemical peel. Image : Rooks textbook of dermatology
Procedure of a chemical peel
Chemical peels are not meant to work just on their own. One has to be motivated to follow a strict skin care plan for the maximum benefits from such a procedure.
A dermatologist will take a detailed history and clinical examination to assess if a patient is a good candidate for chemical peels.
A patient will be counselled on the skin care measures that needs to followed prior and after the procedure as well as about the expectations from this cosmetic procedure.
A process called “priming” which is done to thin out the epidermis so as the acids used in the chemical peel can penetrate the layers of the skin evenly. This step involves daily application of creams containing either retinoids/ azaelic acid/ kojic acid etc for at least 2-4 weeks prior the chemical peel procedure.
Sunscreens is an absolute must before and after the procedure.
A dermatologist may do a test peel behind the ear or other areas just to check if a patient is allergic to any of the ingredient or to assess for potential side effects.
Chemical peels are done in an office based setting once in a 3-4 weeks for 6-7 sessions depending on a patient’s response. The chosen acid is applied to the entire face or target area using a brush after degreasing the face. The peels are left for a certain contact time which is increased every session ( for eg, for the first session the contact time maybe 2 min which is then increased by a minute or two every successive session).
Post peel care
This step is just as important as the actual peel procedure.
Cold compression using ice packs if there is any redness after the prcedure.
Strict sun protection using broad spectrum sunscreens.
Use mild cleansers or soap free cleansers for washing the face.
Use a moisturiser at least twice daily to help reduce the peeling of the skin.
Avoid facial waxing, threading, facials and skin bleaching procedures for at least 1 week after the procedure.
Avoid scratching, picking or peeling of the skin.
Complications
Chemical peels are not free form side effects, that’s why pre procedure counselling and right patient selection is very important.
The possible side effects are :
Persistent redness of skin
Post inflammatory hyper or hypo-pigmentation (i.e dark or light spots)
Scarring
Excessive peeling of skin
Scabbing
Allergic reactions.
Scabbing.
Chemical burns (left) and post inflammatory hyperpigmentation (right) as complications of chemical peel. Image : Rooks textbook of dermatology
Chemical peels are add on cosmetic procedures that can be used for various indications. The effects can be impressive when done by an experienced dermatologist and when a patient is compliant with the pre and post peel skin care.
Never try to attempt a self chemical peel at home with products that can be bought online because the side effects could be permanent if sub optimal products are used and with inexperienced hands.
The beauty standards of this world fuelled by unrealistic expectations through social media has made the slightest blemishes on the skin an un-welcomed sight.
The world is more forgiving towards skin blemishes now, luxury brands are embracing models with vitiligo, freckles have made their way into instagram filters and I personally love seeing this change.
I’m hoping this post will help individuals understand why freckles occur and hopefully help one embrace them.
What are freckles?
Ephelides the medical term for freckles are small unform light brown pigmented areas (maucles) usually occurring on sun exposed skin such as the cheeks, bridge of nose or over the hands.
They are commonly seen in fair skinned individuals with red hair and blue eyes. Freckles can also occur in Asian and Indian skin type though with lesser prevalence.
In an Indian study of pigmentation disorders in Indian skin type, melasma was the commonest cause and freckles only contributed to ~7% of the study population.
Freckles usually start appearing in childhood & adolescence period.
What causes freckles?
Genetics plays a huge role, mutation of a gene encoding for melanocortin receptors have been found especially in red haired individuals. A positive family history of freckles is usually present.
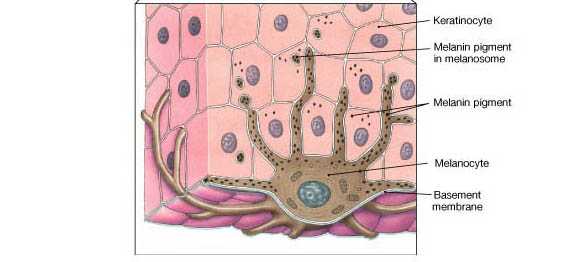
UV radiation stimulates the melanocytes to produce more melanin (the pigment of our skin) and it also increases the transfer of the melanin to the keratinocytes (cells of the upper layers of our skin) and is responsible for the pigmenation.
The number of melanocytes (specialised cells in the skin that makes the pigment melanin) are not increased but there is an increase activity of these melanocytes.
For an individual who is genetically predisposed, UVR (sun exposure) can cause the development of freckles
Freckles appear at early childhood (2-3 years) over the cheeks, nose or the hands.
They are light brown, 1-5 mm in size, round to oval, regular & well defined patches. Freckles are mostly uniform in size, colour and distribution.
They become darker on sun exposure and fade with strict sun protection. Hence they tend to be more prominent in summer and lighter in winter.
They may even fade with age.
Solar lentigens / Sun spots
Image credit : DermNetNZ
Starts appearing in adulthood 20-30 years.
Light -dark brown patches on the sun exposed areas such as face, upper neck, hands. They are larger & more irregular than freckles.
Can occur both in light and dark coloured skin.
Caused by prolonged sun exposure over time.
They become darker with more sun exposure and do not fade in winter. They are persistent throughout life and no not fade with time. They may even increase in number with age.
When to worry about freckles?
A child with multiple freckles and a severe intolerance to sunlight
If the child develops severe sun burns even with minimal sun exposure, a detailed medical examination may be required to rule out genetic disorders such as xeroderma pigmentosa where the cells fail to repair the DNA damaged by UV radiation.
Are freckles harmful?
Freckles are completely harmless unless if its associated with the above mentioned condition.
How to fade freckles?
Freckles respond well to strict sun protection either in the form of sunscreens or physical protection.
I’ve mentioned in my previous blog posts on how to achieve a good level of sun protection.
Other form of treatments are topical creams such as hydroquinone or retinoids. However these tend to give an uneven result.
Chemical peels have shown good results, such as spot TCA or Phenol peels. In these procedures, a high strength alpha hydroxy acid (glycolic acid, mandelic acid etc) or caustic acid (TCA)are applied by a dermatologist using a toothpick or cotton buds to the freckles. These areas then forms a scab with falls off in 7-10 days and heals with a normal pigmented skin.
LASERS have been widely used successfully for fading the freckles as well.
All the above procedures do come with certain side effects such as irritation, redness, pigmentation (especially in dark skinned individuals). Therefore always find a dermatologist experienced in this field to perform such procedures.
Recurrence of the freckles or sun spots can occur hence strict sun protection must be maintained even when the freckles have faded.
My advised is, start loving your sunscreen, use it judiciously for best results.
Try the other treatment options if you are very concerned about the freckles but in my opinion, every blemish, or scar or mole adds character to your face, learn to embrace it.
As I was growing up I’ve seen my mum and most of my aunts trying in vain every remedy available for the pigmentation on their face
What is melasma?
Melasma also called cloasma is a common acquired hyperpigmentation disorder affecting mostly women in their reproductive age groups (~15-45 years) . It is the most common pigmentation disorder & is seen more commonly especially in individuals with darker skin type (FST IV-VI) affecting 9 -50% of the such high risk population . (Find out your skin type here)
What causes melasma?
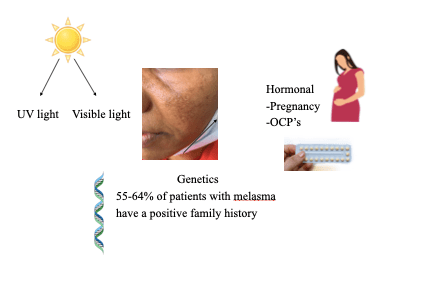
Cause of melasma is multifactorial and factors such as UV radiation, elevated estrogen (female hormones) level work together to result in melasma in genetically predisposed individuals
Genetics: Certain genes are responsible for up regulating enzymes in the melanogenesis pathway (process of melanin production) which results in more melanin production.
UV Rays: Increase production of reactive oxygen species, which can then increase tyrosinaseactivity.
Hormones: Estrogen can up regulate enzymes (tyrosinase) and genes in the melanogenesis pathway, resulting in increase pigment production in genetically predisposed individulas.
How does it present?
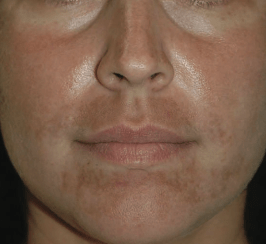
Melasma presents with tan brown reticulate (lacy) pigmentation described in three distinct pattern on the face.
Centro facial pattern: Most common pattern affecting the forehead, nose, upper lip, chin and cheeks
Malar pattern : As seen in the below images affects the malar area (cheeks) of face
Mandibular pattern: Affects the jawline and chin, mostly seen in late onset melasma
Melasma in women can present for the first time in pregnancy and its referred to as “Mask of Pregnancy“. Treatment of which is more difficult because of the increase estrogen level in the body and as most medications used for pigmentation may not be safe during pregnancy.
The good news is that in some women, this mask of pregnancy is transient and will fade with time and proper management.
Can melasma occur in males?
Yes, melasma can occur in males as well. The male to female is ratio 1:9 i.e for every 9 females with melasma, 1 male individual also suffers from melasma. It has also been reported to have a higher prevalence in Indian males compared to Caucasian males.
Does melasma occur elsewhere besides the face?
Yes, rarely it can involve the neck, chest, the upper arms or forearms and it’s called “Extra facial melasma”
How is it diagnosed?
Most of the time a dermatologist can diagnose melasma by just examining it.
A wood’s lamp examination may be used to assess the dept of the pigmentation i.e if it is epidermal (superficial) or dermal (deep) pigmentation. Epidermal pigmentation respond to treatment better.
Occasionally a skin biopsy (examining of a skin sample under a microscope) may be required for a definitive diagnosis as all facial pigmentation is not melasma.
Treatment options
The hunt for the cure for melasma is still ongoing.
Though numerous treatment options are available now, there is still no “one product” that does it all.
The mainstay of treatment is avoiding the factors responsible for it as much as possible. Since one cannot change one’s genetic makeup, taking measures to avoid the modifiable factors (such strict sun protection) will help prevent its occurrence and reduce the appearance of an already developing melasma.
Its always good to know your personal risk of developing melasma so as you can actively prevent it from occurring in the future.
If melasma is highly prevalent in your ethnic group (for eg: melasma is highly prevalent in my hometown i.e Shillong, Northeast India) start taking preventive measures at the earliest. Its best to consult a dermatologist as early as possible at the start of the pigmentation rather than after a trail and error of using multiple self prescribed creams and remedies.
Shillong, though blessed with its hills, rivers, waterfalls and clouds, being at a higher altitude (1525 m above sea level) means it gets more UV rays than lower altitude areas and the cloud cover aids in scattering these UV rays. Understanding these facts will help individuals be more aware of the need of sun protection even in cloudy, pleasant days without the sun shining bright.
The first step to the treatment or prevention of melasma is strict sun protection. No creams, chemical peels or LASERS will effectively work if one is not complaint with this step
Gel formulation or matte finish for those with oily skin
Apply to both face and neck at least 20 mins prior to sun exposure and reapply every 2 hours especially when outdoors
Sunscreen application should be on all days even when the sky is cloudy or rainy
Use a sunscreen even when indoors (as glass cannot filter UVA light)
Other measures of sun protection include using a wide brim hat during your outing tot he beach or during any outdoor activity.
Avoid the peak hours of the day such as between 12 noon -2 pm when the sun is directly above the earth.
Seek shade whenever possible
Treatment to reduce pigmentation
Now that we’ve had sun protection covered, you will need to seek expert opinion (dermatologist) for further management as there are many active ingredients available for treating pigmentation and not everything is suitable for everyone.
If you are on medications such as oral contraceptive pills containing estrogen or drugs for seizures such as phenytoin which could be the potential cause of the melasma, then its best to speak to your treating physician for a possible changeover of the medications.
What are the treatment options available?
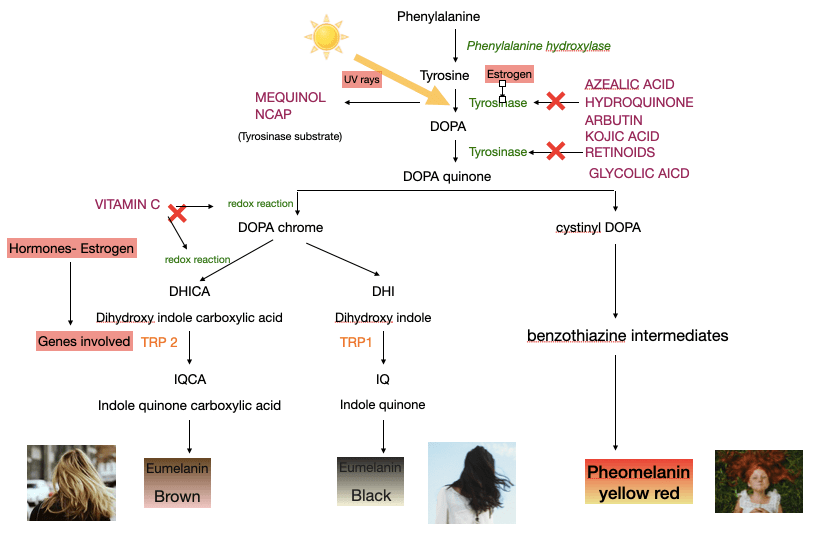
To understand how the treatments work, we first need to have an overview of how melanin (pigment responsible for our skin, hair, eyes colour) is formed.
Melanogenesis i.e process of melanin formation in melanocytes (cells for melanin production). The 3 main types of melanin are eumelanin brown, eumelanin black & phaeomelanin (yellow red). Humans have all 3 types but the ratio of each type of melanin is different in different ethnic group. For eg more pheomelanin is present in red heads with pale fair skin, more of brown eumelanin is seen in blondes and more of eumelanin black is seen in brown-black skin type with black hair.
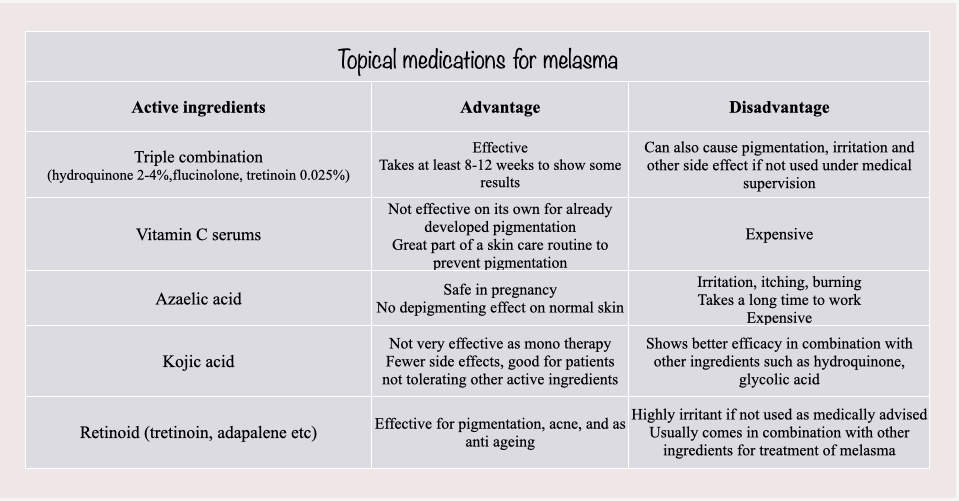
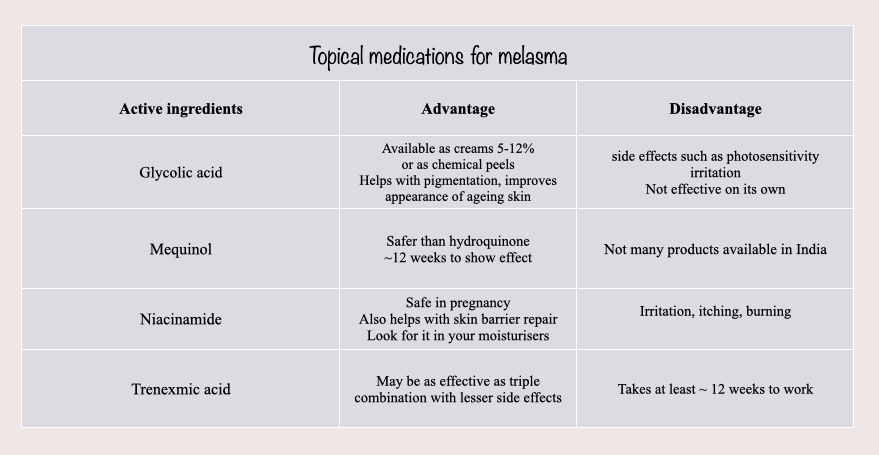
Topical medications for melasma
Various options are availabe in the form or creams, ointments or serums and the choice will differ from patient to patient.
Topicals required long term and consistent use for the best results.
Not every option will work for everyone
Some of the active ingredients that are use to reduce pigmentation are enumerated in the tables below:
There are numerous options for the treatment of melasma, and the choice will depend with every patient.
For best results, sun protection, strict compliance and abundance of patience is required as improvement can only be appreciated after months of consistent skin care routine.
Oral medications for melasma
Trenexamic acid – An anti fibrinolytic drug that prevents the breakdown of protein (fibrin) present in blood clots. Therefore it is traditionally used to treat bleeding disorders.
It has been shown to be effective for the treatment of melasma in low doses. It has been show to produce results in 3 months but relapse rates are high and melasma recurs within 3 months of discontinuation of the drug.
Side effects are nausea, vomiting & serious side effects such as heart attacks, blood clots in veins of legs, renal injury (kidney problems) could potentially occur in individuals at risk.
Chemical peels
Dermatological procedure where acids of higher strength is used such as glycolic acid, salicylic acid, trichloroacetic acid etc are applied to the face or pigmented area by a dermatologist for a short contact time.
The procedure is done every 3-4 weeks for 5-6 sessions depending on the patient’s response.
Second line treatment for those not responding to topicals alone.
Expensive and requires an experienced hand.
LASER for melasma
Various types of LASER are available for the treatment of melasma.
LASER treatment can be tricky especially in individual’s with darker skin type as the risk of pigmentation is higher. LASER are usually reserved for resistant cases not responding to the above mentioned treatment options.
LASER are not one time treatment. Creams and sunscreens will still be required to maintain the result and prevent recurrence.
LASER treatment are expensive but may be worth it when done by experienced hand.
There is still no cure for melasma.
Seek guidance from a dermatologist as the appearance of the pigmentation can be improved with either depigmenting creams & sunscreens or a combination of treatment especially when the treatment is started early.
Acne is such a common condition that to an untrained eye, all red bumps (papules/pustules) must be acne.
There are other dermatological disorders that present like acne but are not acne.
Pityrosporum folliculitis or Malassezia folliculitis (Fungal acne in layman terms, but fungal acne is not a medical diagnosis since it’s not acne or form of acne) is one of the most common skin condition mistaken for acne. It is caused by increase colonisation (multiplication) of a yeast called Malassezia species which is normally present as part of the normal flora in our skin. (yes! our skin has a world of micro organisms living in it 😉 )
It is the inflammation caused by such an increase colonisation that causes the symptoms.
So what causes this increase colonisation by this yeast?
Malassezia thrives in the oily environment produced by the sebaceous glands. Adolescents (10-19 years) have an increase sebaceous glands activity due to the hormonal fluctuations. Therefore this condition is commonly seen in adolescents.
Excessive sweating is also a risk factor, and people living in hot humid areas are more predisposed.
Individuals on topical or oral antibiotic, as this can suppress the growth of the normal bacteria in the skin giving way for this yeast to multiply unchecked.
Use of steroids or other immunosuppressant agents.
Diabetic patients may also experience such eruptions.
Genetic predisposition also plays a role. As mentioned earlier everyone has this yeast in their skin, but only some people are able to mount an inflammatory response to it causing the symptoms while others do not.
How can you differentiate it from acne ?
Firstly by the looks of the lesion, fungal acne presents with monomorphic (uniform looking) papules (red raised bumps) or pustules (pus filled bumps). There will not be any comedones (such as white heads or black heads) unless a patient also has concurrent acne.
Secondly by examining the site of involvement, face (forhead), back, upper arms, chest and back are involved in fungal acne. One wouldn’t normally see acne vulgaris involving the upper arms, neck.
Thirdly, fungal acne tends to be itchy while acne is not. Do you ever remember your pimple itching unless you’ve picked on it and a scab has formed?
Fourthly, history of acne not responding to anti acne treatment despite strict compliance or acne which had responded to treatment and suddenly flares up even while on the same treatment.
Fifthy, individuals with fungal acne may also have dandruff or tinea versicolor.
Do you need to see a dermatologist for such a condition?
Its always better to get an expert opinion before you self treat any skin condition.
Though the above points can help distinguish between acne and fungal acne, it may not be as clear cut in most cases, especially when one also has co existing acne. A variant of acne called truncal acne vulgaris can also present with similar eruptions on the back and chest.
Another dermatological condition called acneiform eruption which presents as eruption of skin lesions similar to acne caused by certain medications, mechanical friction, certain compounds used in textile dyes, insecticides, pesticides, detergents or soaps (halogenated aromatic hydrocarbon) presents similar to acne, and is sometimes difficult to differentiate it from fungal acne.
This is where a dermatologist’s opinion is important, so that certain questions can be asked, and if necessary certain tests performed (such as Wood lamp examination or KOH mount which can help in the diagnosis of fungal acne) for the correct diagnosis and management of the condition.
How to treat it?
As it is seen that the organism causing fungal acne (i.e Malassezia sp) can multiply more in hot and humid areas and summers are the season for most flare ups due to the increase ambient temperature and sweating, measures to reduce these factors can help reduce the symptoms
Have frequent cold showers in the summers
Change clothing such as gym wear, uniforms as soon as possible
Opt for loose fitting clothing
Avoid tight fitting attire
Seek the comfort of an air conditioned room
Products to use :
Use an anti-fungal shampoo (such as 2% ketoconazole or selenium sulfide or zinc pyrithione), look out for these ingredients in your anti dandruff shampoos. (List of few of such shampoos on previous post)
2% Ketoconazole + zinc pyrithione
Zinc pyrithione
Zinc pyrithione
Massage the shampoos to the affected areas and leave it for 5-10 mins and wash off. This can be done twice weekly for at least 2-4 weeks depending on your response.
If the above fails, your dermatologists may add topical anti-fungal creams which are to be applied once-twice daily over the lesions.
Topical creams that helps to unclog the blocked sebaceous glands such as salicycic acid is another adjunctive treatment option in addition to the above.
Systemic anti-fungals (oral tablets/capsules) may be required in some cases.
Remember that the condition may recur, especially in summers.
Applying the anti-fungal shampoos during the summer months once weekly even if you don’t have the flares may help reduce chances of recurrence
We have all, at one point in time, dealt with excessive hair fall that alarmed us enough to either self treat with DIY/home remedies or to seek a dermatologist’s opinion.
Let us understand the normal physiological process that our hair goes through which is called “Hair cycle”.
Hair cycle is divided into 3 main phases :
Anagen (90% of the hair are in this active growing phase ) which proceeds to:
Catagen (resting phase), which then progress to :
Telogen (regressing phase)–> the hair then eventually falls out (exogen) as the hair follicle enters a new anagen phase.
As you can see that as new hair grows, the existing hair in that particular hair follicle has to fall out. So hair fall should not necessarily alarming, and this normal hair shedding is seen to be 50-100/day and in some individuals it could be upto 150/day as well.
When to seek a dermatologist’s opinion?
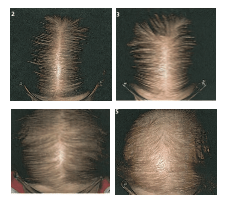
When the hair fall exceeds what was mentioned above, or you start noticing recession of the hair line or thinning of hair in crown (in men), thinning of the hair and a more visible scalp along the part line (in females), or patches of hair loss.
Common causes of hair loss:
1. Telogen effluvium: Presents with a more diffuse hair loss of >150/day. Occurs 2-4 months after any systemic illness such as infections (malaria, typhoid etc), childbirth, surgeries, crash diet, thyroid disorders, psychological stress etc.
The condition is completely reversible and the hair loss starts improving in 4-6 months once the underlying factor is corrected.
Female pattern hair loss
2. Androgenetic alopecia ( also called male pattern baldness or female pattern baldness in men & women respectively due to the characteristic pattern of hair loss). It is genetic disorder, in which susceptible hair follicles either have a higher response to the hormone testosterone, or have a higher amount/activity of the enzyme ( 5 alpha reductase) which converts testosterone into a more active form.
Male pattern hair loss
This result is the normal terminal hair (thick , black scalp hair) is transformed into vellus hair (thin, fine, light coloured hair mostly found in other parts of our body).
The overall effect is gradual thinning of hair. The disorder can be inherited from either maternal or paternal side
Image: DermNetnz
3. Traction alopecia:
Caused by the excessive constant stretching of the hair shaft from hair styling such as tight braids/ ponytails
4. Alopecia areata: Considered an autoimmne disease normally seen in children and presenting with localised patches of hair loss, rarely it can affect adults and be of a more diffuse nature.
Usually self limiting i.e hair regrows back even without treatment.
There are more causes of hair loss, but the ones mentioned above are the commonest ones experienced by individuals.
Treatment for the different types of hair loss may vary with some requiring no specific treatment at all such a telogen effluvium whereas others have specific therapy such as alopecia areata and androgenetic alopecia.



















































{kind=link}
{kind=link}